The 10 Pillars of Professional Practice: Moving Beyond Fitness with a Medical Flavor
To transition fitness professionals from a "workout-centric" mindset to a system-driven, professional practice model by mastering the 10 key concepts of Medical Exercise Training.
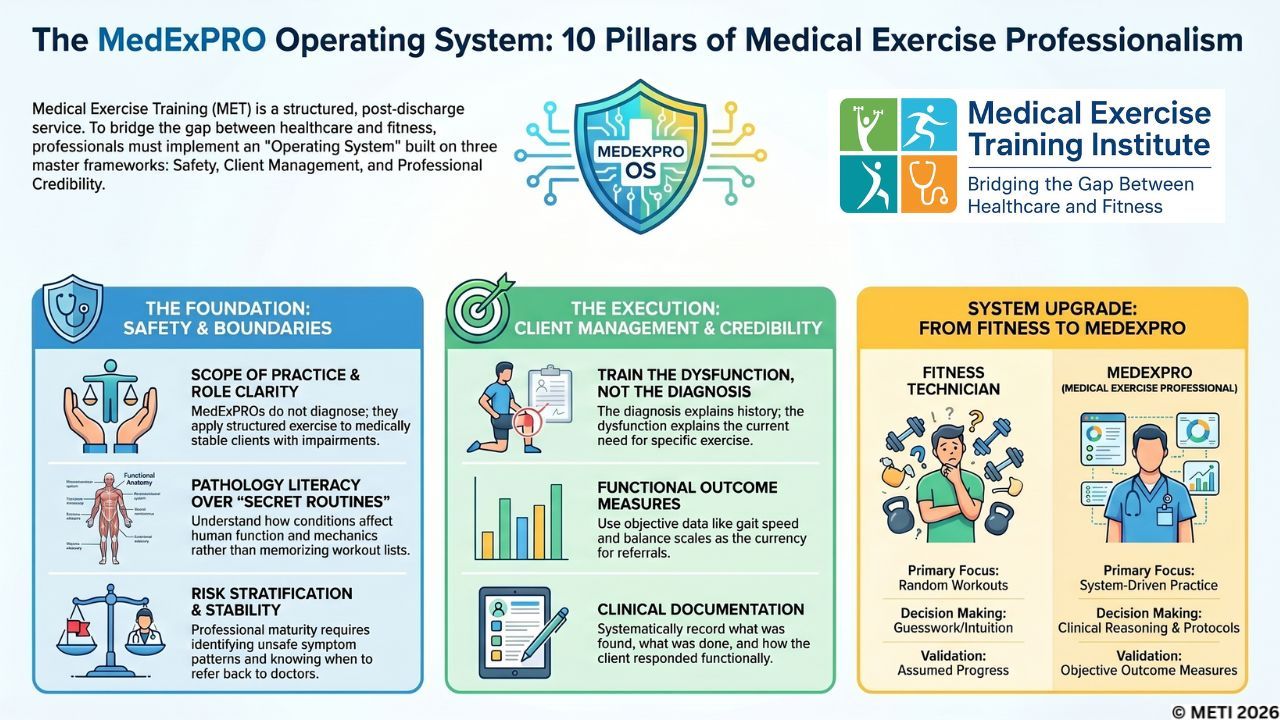
Medical Exercise Training (MET) is not general fitness with a medical flavor. It is a structured, post-discharge, exercise-based professional service. To earn medical referrals and build a sustainable practice, the Medical Exercise Professional (MedExPRO) must move from technician thinking to professional practice ownership by installing systems for safety, client management, and professional credibility.
Professional Standard
Many fitness professionals believe that working with clients who have medical conditions simply requires knowing a few extra exercises. They look for the "secret routine" or a collection of specialized workouts.
But medical professionals do not refer to routines. They refer to systems.
If you want to bridge the gap between healthcare and fitness, you must move beyond the mentality ...
Medical Exercise Training eBook Tip 52: How & When to Discharge A MET Client
Welcome back to the MET 101 eBook series! In Tip 52, Dr. Mike addresses a transition that separates general personal trainers from true Medical Exercise Professionals (MedExPROs): How and when do you discharge a Medical Exercise (ME) client?
If you want to be fully integrated into the healthcare network, you must understand that ME clients are not meant to stay ME clients forever.
The Goal is Independence, Not Dependence: The fundamental goal of every healthcare provider—from surgeons to physical therapists—is to get the patient to a point where they no longer need intensive care, requiring only supervision or periodic check-ins. The exact same holds true for MedExPROs.
A trap that many fitness professionals fall into is wanting to hold onto a medical exercise client indefinitely because they can charge a higher premium for those specialized services. However, once a client's function, power, strength, and proprioception have significantly improved, they no longer require the advanc...
Why So Many MedExPROs Struggle to Grow a Strong Practice—And What to Do About It
Most Medical Exercise Professionals do not fail because they lack passion, care, or technical knowledge.
They struggle because they are trying to grow a practice without a clear structure behind it.
They know how to work hard.
They know how to help people.
They know their clients need them.
But behind the scenes, too many MedExPROs are still asking the same questions:
What should I be documenting?
How do I communicate with physicians, physical therapists, and chiropractors?
How do I make my services easier to explain?
How do I attract the right clients?
How do I build a practice that feels organized, professional, and profitable?
That is where the real problem begins.
A lot of good MedExPROs are delivering solid service, but their practice still feels scattered. Their message is unclear. Their systems are inconsistent. Their documentation is weak. Their communication is irregular. Their pricing may not reflect the value they provide. And because of that, growth feels harder than ...
"Are You Just Exercising, or Are You Restoring Function? How to Shift From Technician to MedExPRO"

Mrs. Jacobs, Your New Client, Walked In With a Walker...
Here’s How to Go from Trainer to Real MedExPRO
Mrs. Jacobs is 79.
She’s 4 months post-total hip replacement (THR). She also has a history of total knee replacement on the opposite side.
While she can:
- Walk independently on level surfaces with her walker
- Climb stairs independently
She struggles with:
- Fatigue in her lower extremities
- Inability to stand for long periods
- Walking for more than 10 minutes without tiring
She’s also managing:
- Hypertension
- Mild Parkinson’s disease
- Osteopenia (bone thinning)
Her Goal:
Mrs. Jacobs’ ultimate goal is to discontinue the walker and be able to walk into the grocery store and shop without limitations.
She is scheduled to see her orthopedist in 45 days and her **primary care physician at the end of the month.
Do you know what to do, when to do it, how to progress her and how to communicate with her medical providers….if you don’t…keep reading.
So, What Would You...
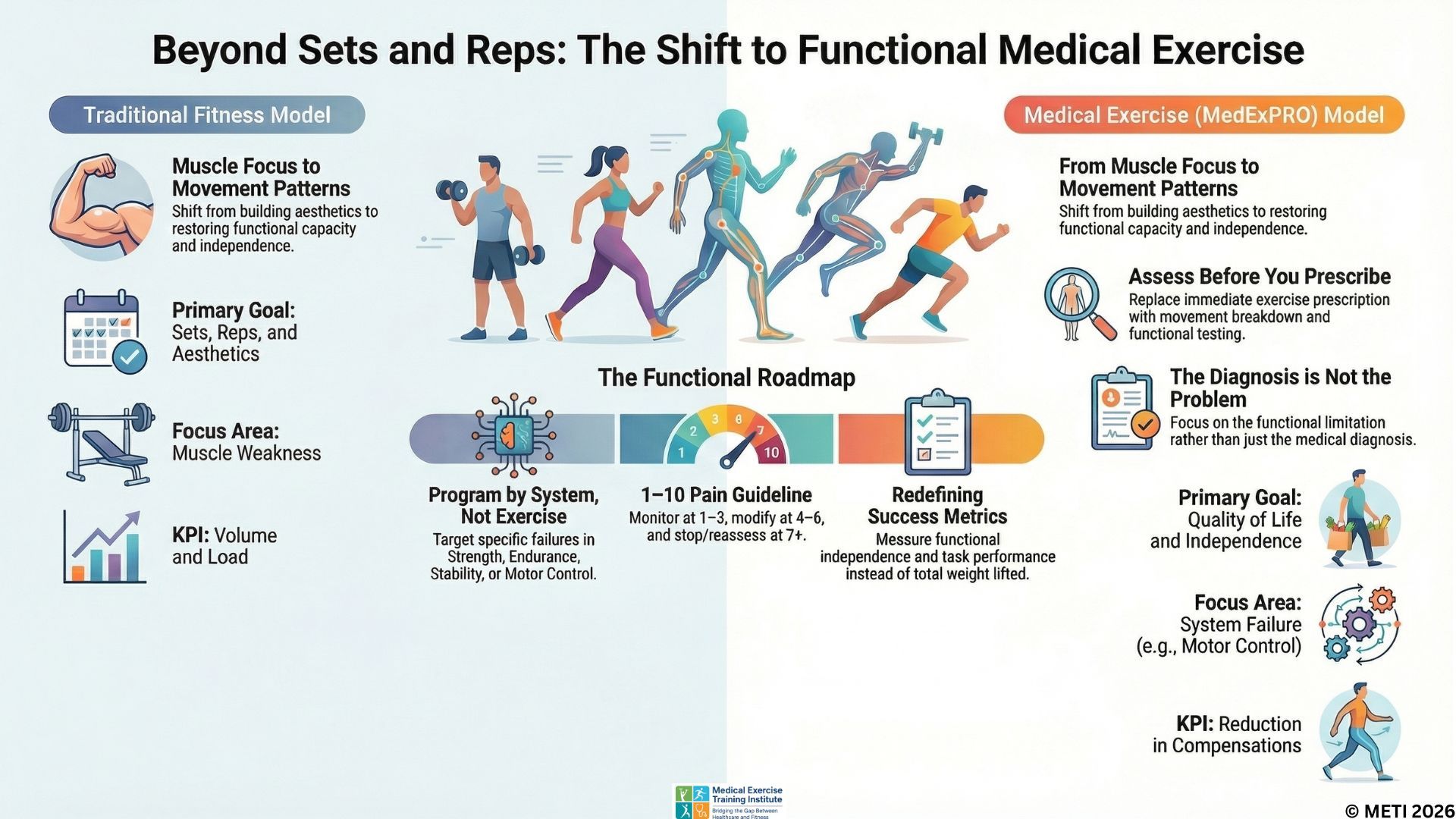
Beyond Sets & Reps: The MedExPRO Guide to Functional Medical Exercise
The Problem No One Is Addressing
Let’s cut to the chase.
The fitness industry is still obsessed with counting reps. Meanwhile, healthcare is discharging patients too early, leaving a massive gap in the continuum of care.
And who’s falling through the cracks?
The clients who:
- Have been “cleared” after therapy
- But still struggle to function in their daily lives
They may have completed physical therapy, but they:
- Struggle to get out of a chair
- Walk with instability
- Fatigue quickly
- Avoid movement because of pain or fear
This isn’t a strength problem—it’s a functional breakdown problem.
And here's the key point:
No one outside of properly trained Medical Exercise Professionals (MedExPROs) is equipped to solve it.
Beyond the Workout: The Real Role of the MedExPRO
Here’s the reality—most fitness professionals ask:
"How many sets and reps?"
But as a Medical Exercise Specialist, you should think BEYOND SETS & REPS:
“What function is missing—and why?”
That small shift i...
MedExPRO….Do MET Clients Stay Clients Forever? Understanding Functional Maintenance
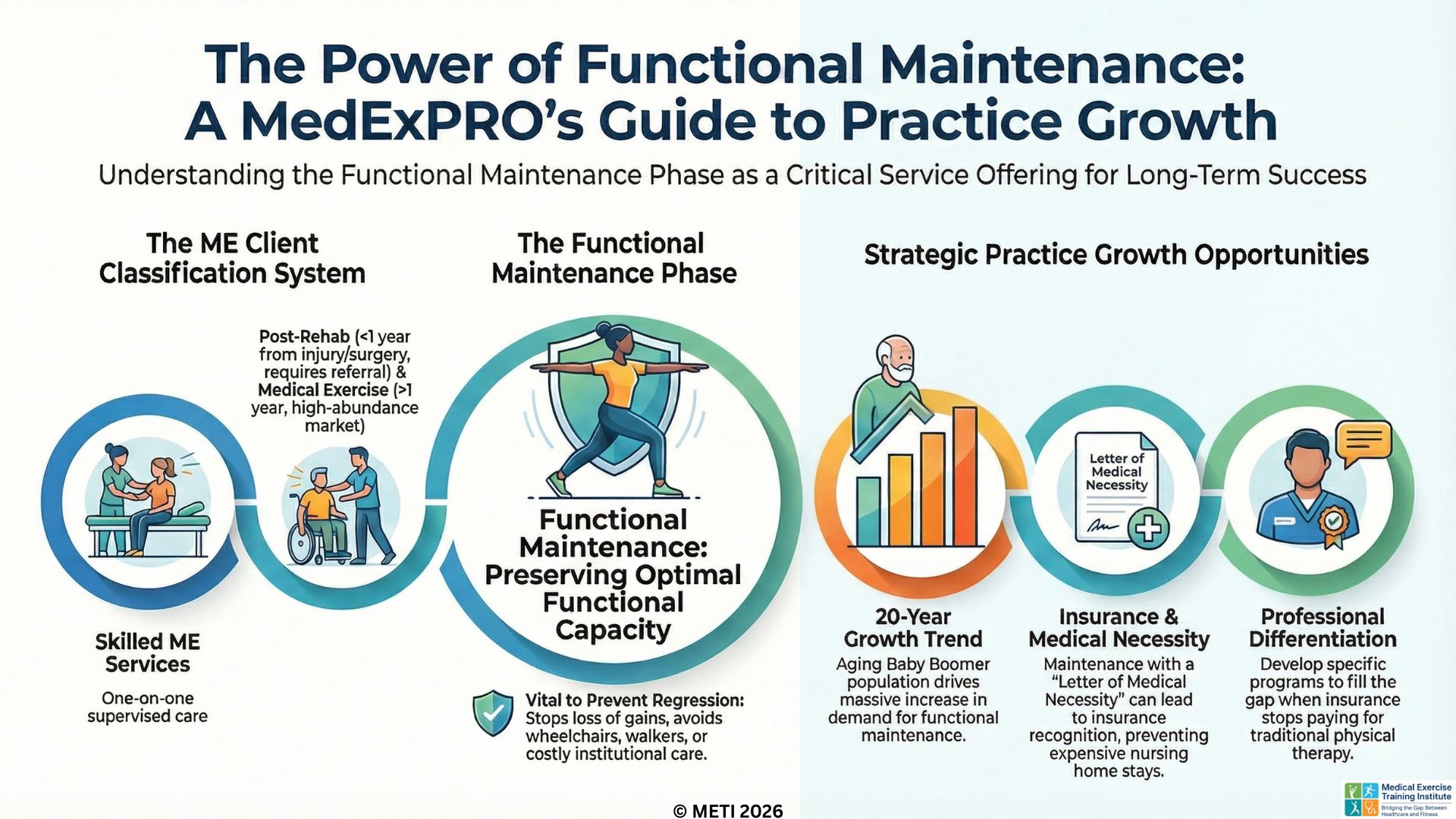
Welcome back to the MET 101 eBook series! In Tip 51, we address a very common and important question for Medical Exercise Professionals (MedExPROs): Do MET clients remain MET clients forever?
The short answer is no. Just as medical treatment eventually concludes, skilled MET services—which involve intensive one-on-one or group-based supervision—also reach a conclusion. At a certain point, a client achieves their optimal functional capacity and no longer needs primary MET services. When this happens, they transition into a critical phase known as Functional Maintenance.
The 4 Post-Rehab Client Classifications: To understand where Functional Maintenance fits in, it helps to understand the four primary classifications of clients you will see in your practice:

- The Post-Rehab Client: This client has sustained an injury, undergone surgery, or been diagnosed with a condition within the last year. They always require a medical referral before you begin working with them.
- The Medical ...
MedExPRO - Neck Pain Isn’t Just Pain—It’s Lost Function—Can You Measure Functional Improvement
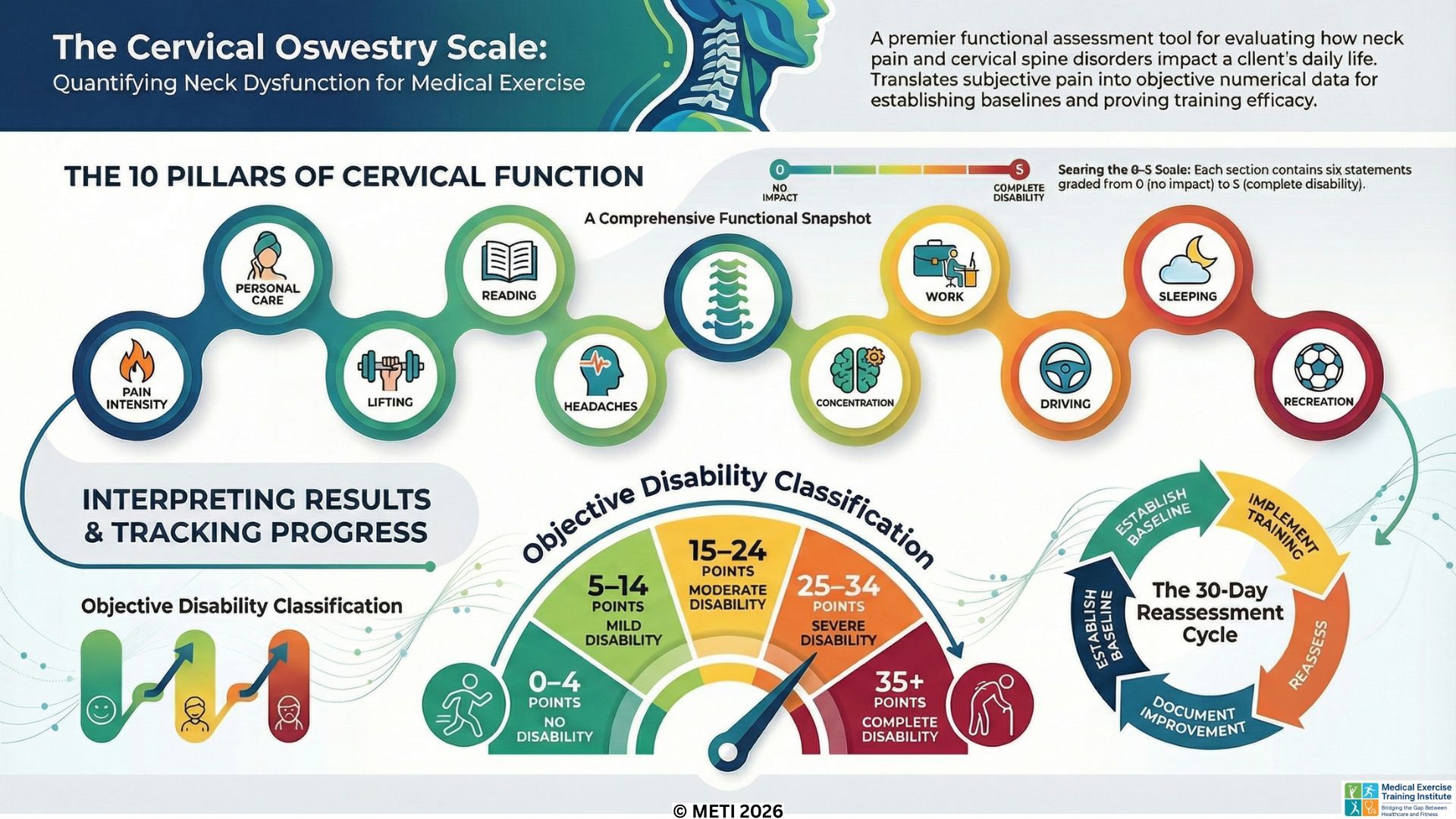
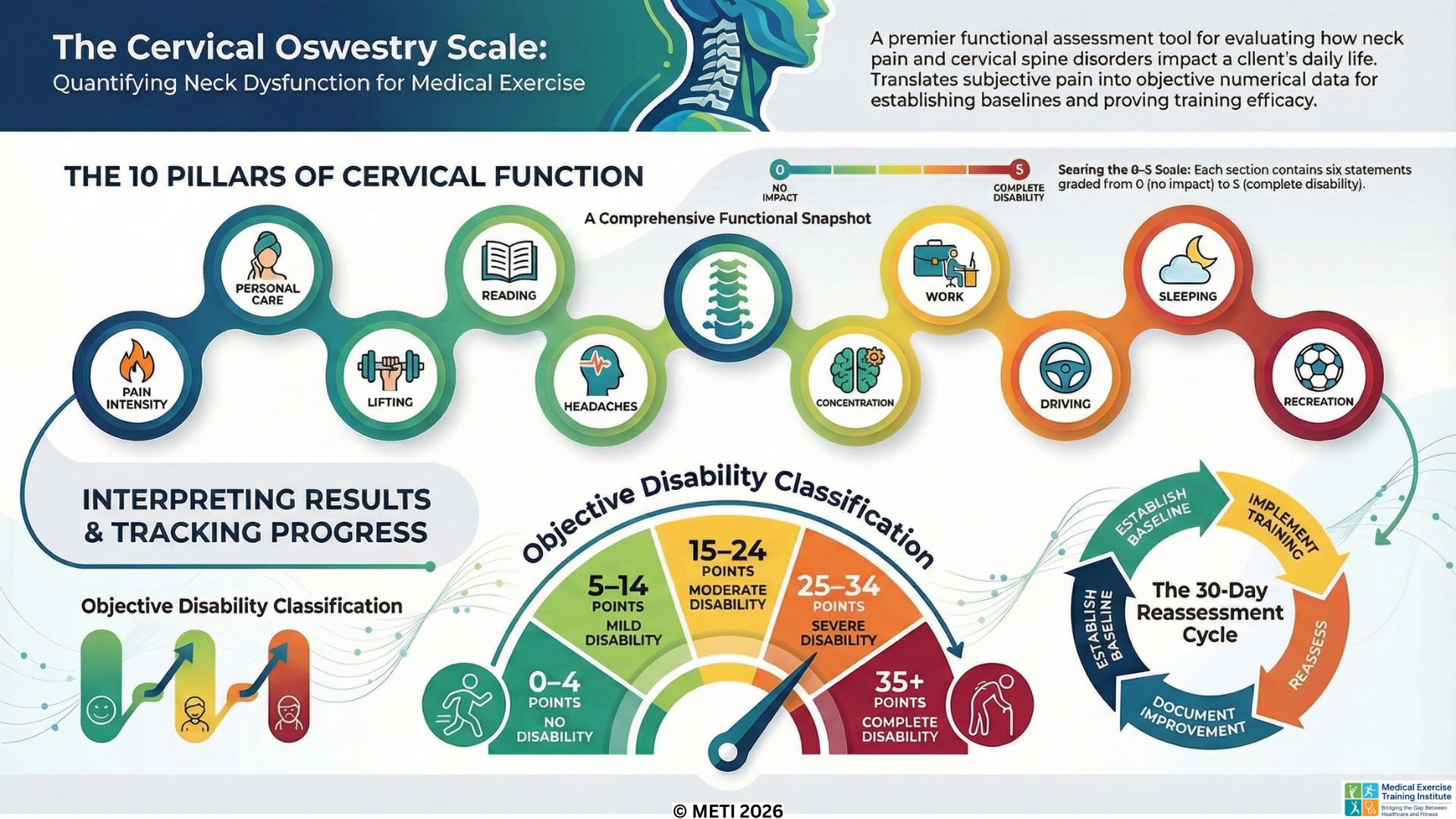
The Cervical Oswestry Scale: Measuring the True Cost of Neck Dysfunction
Just as the Lumbar Oswestry Scale measures lower back dysfunction, the Cervical Oswestry Functional Assessment Scale is the premier tool for evaluating clients with cervical spine disorders. Also developed by Dr. Gordon Waddell, this questionnaire-based scale takes a comprehensive "snapshot" of how neck pain, stiffness, and cervical limitations impact a client's overall lifestyle and daily activities. For Medical Exercise Professionals (MedXPROs) managing conditions like cervical strain or disc herniations, this tool is vital for setting baselines and proving program efficacy.
Get the Podcast Here
The Cervical Oswestry Scale consists of 10 specific sections, each containing six statements graded from 0 to 5. The sections cover Pain Intensity, Personal Care, Lifting, Reading, Headaches, Concentration, Work, Driving, Sleeping, and Recreation. This scale is uniquely tailored to the symptoms most frequently assoc...
Medical Exercise Specialist Snapshot of Lumbar Function
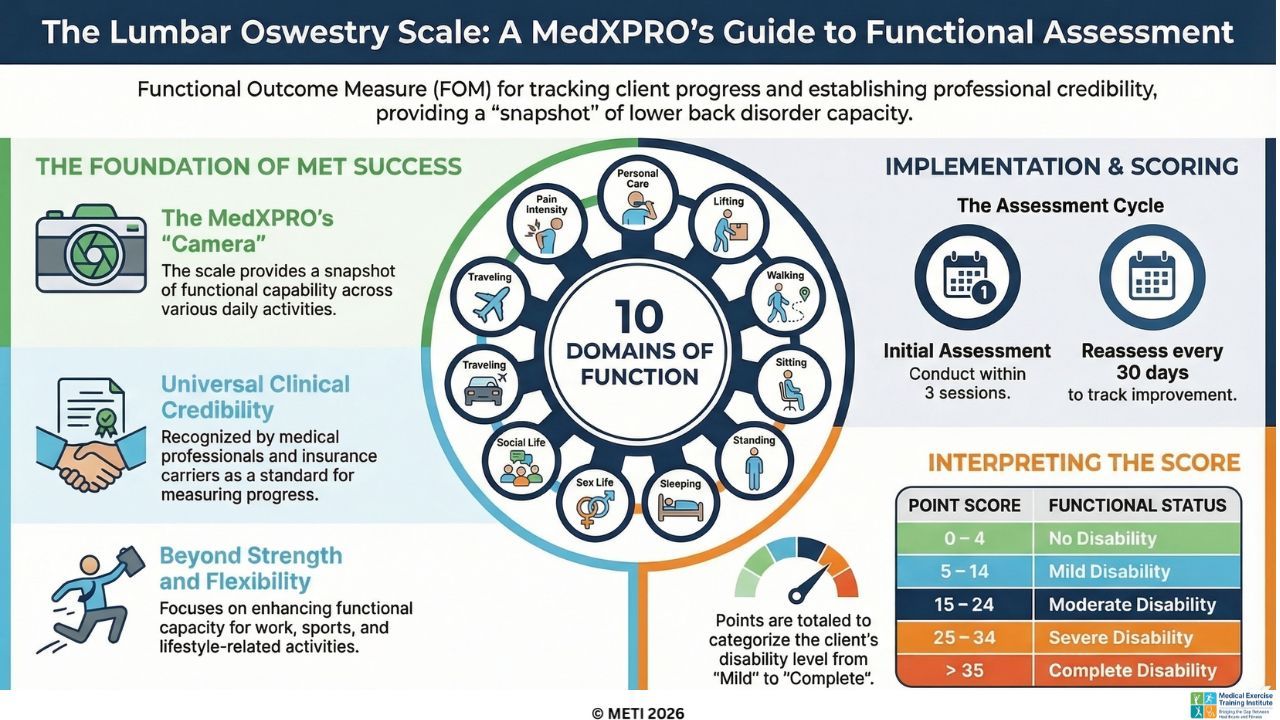
For Medical Exercise Professionals (MedXPROs) managing clients with low back pain and lumbar spine disorders, the Oswestry Lumbar Scale is an indispensable functional assessment tool. Developed by Scottish industrial rehabilitation physician Gordon Waddell, this scale translates the subjective experience of back pain into a concrete, objective numerical value. Rather than merely testing a client's lumbar range of motion or isolated muscle strength, the Oswestry Scale uses a battery of targeted questions to determine exactly how a lumbar condition impacts a client's daily functional capacity.
The Lumbar Oswestry Scale is divided into 10 distinct sections, each addressing a critical aspect of daily living. These sections include Pain Intensity, Personal Care (such as washing and dressing), Lifting, Walking, Sitting, Standing, Sleeping, Sex Life, Social Life, and Traveling. Within each section, the client selects from six statements that best describe their current level of function or l...
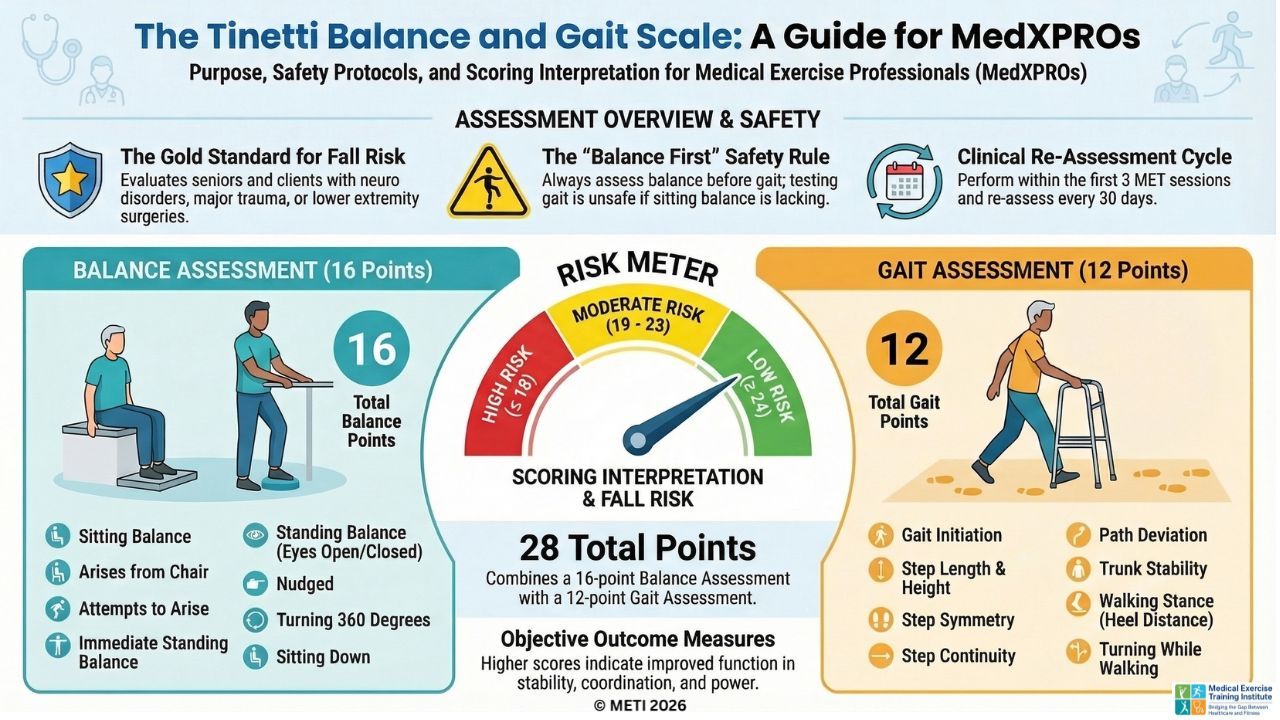
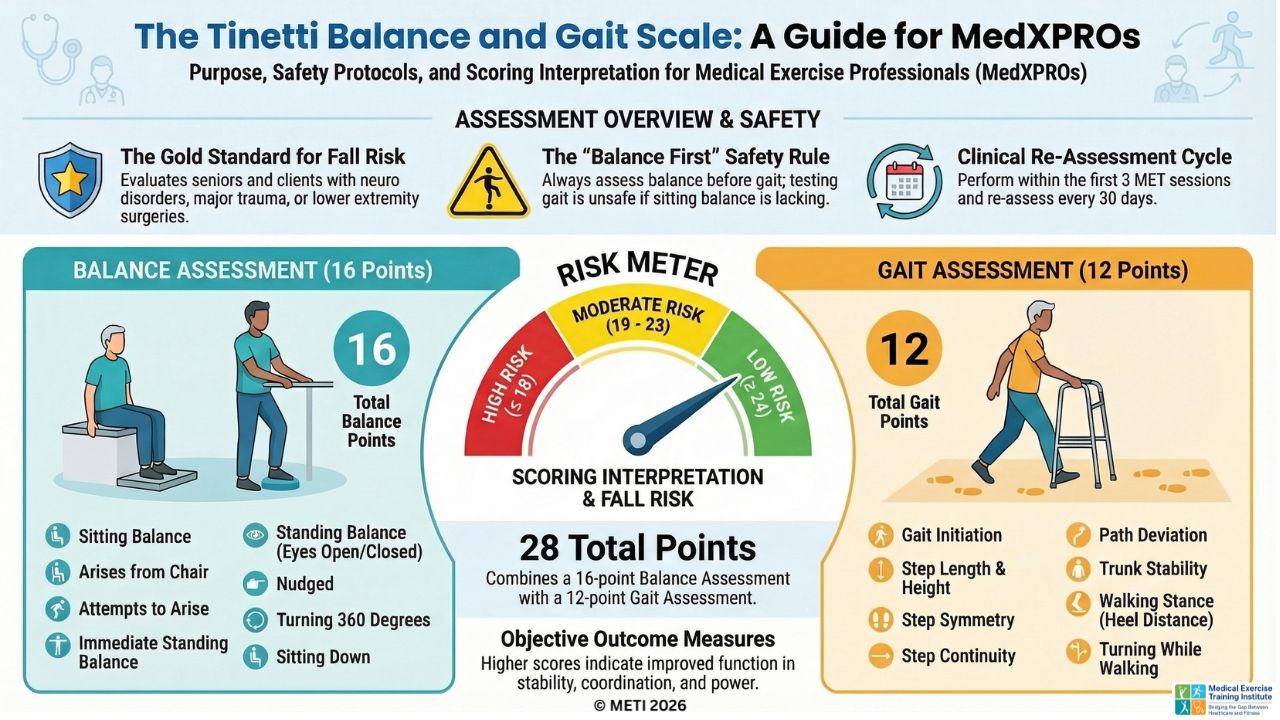
Medical Exercise Training Ultimate Fall Risk Assessment - Tinetti Balance/Gait Scale
Get the Podcast Here
The Tinetti Gait and Balance Scale is one of the most frequently used and critical functional assessment tools for Medical Exercise Professionals (MedXPROs) working with aging populations and those with neurological challenges. Specifically, this scale is ideal for seniors, clients utilizing an ambulatory assistive device, or individuals with a history of a cerebrovascular accident (CVA/stroke), Multiple Sclerosis, Parkinson’s disease, lower extremity surgery, or major trauma. Rather than just evaluating isolated strength, the Tinetti Scale provides a comprehensive snapshot of how a client's body functions in motion and at rest, accurately determining their precise risk for falls.
This objective assessment is divided into two distinct components: Balance and Gait, yielding a maximum combined score of 28 points. The Balance assessment must always be performed first; if a client lacks independent sitting balance, progressing to gait testing may be highly unsafe.
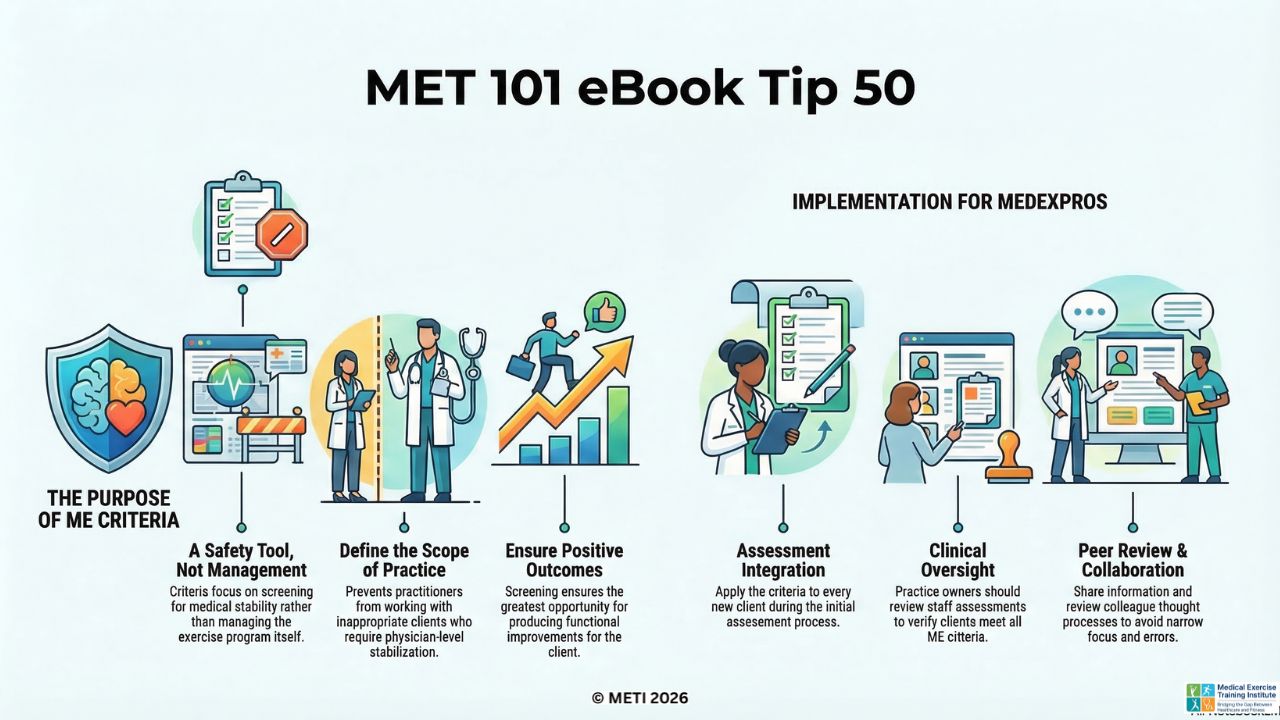
...MET 101 eBook Tip 50 - The Ultimate Guardrail - Why MET Criteria Are for Safety
Why MET Criteria Are for Safety, Not Management
Welcome to a milestone in our MET 101 series! In Tip 50, Dr. Mike tackles a highly anticipated follow-up question regarding Medical Exercise (ME) criteria: How will the MET criteria help me manage my clients?
The answer might surprise you: The criteria will not help you manage the client through the MET program.
Instead, Dr. Mike emphasizes that the criteria are fundamentally a safety tool, rather than a management tool. Their primary purpose is to act as a strict guardrail designed to prevent medically unstable clients from entering an ME program. If a client requires the medical stabilization skills of a physician, nurse, or physician's assistant, working with them falls far outside a MedExPRO's scope of practice and ethical range. Adhering to these criteria ensures you have the greatest opportunity to produce a positive functional outcome, while simultaneously keeping you out of "hot water" and professional liability.
A Crucial N...